













Request a video call
Confirm Your Virtual Consultation
Obesity Bariatric Surgery by Dr. Jorge Maytorena Profile Overview

Table of Content
Dr. Jorge Maytorena is a weight loss doctor. He helps people get thinner. He has done this for 16 years. He is very good at his job. He helps many people feel better. He knows a lot about bariatric surgery in Tijuana Mexico. He uses the best tools to help people. He wants the best for his patients.
His office is in Mexico. Everyone there wants to help you. They want you to be healthy. They will help you before, during, and after your surgery.
Why Choose Bariatric Surgery in Tijuana, Mexico?
Average Cost of Bariatric Surgery in Tijuana, Mexico
The price of weight loss surgery in Tijuana, Mexico, usually costs less than in other countries. On average, it can cost between $4,600 and $5,699, depending on the type of surgery and the clinic. Many people choose Tijuana because the prices are lower, but they can still get good care.
|
Procedures |
Cost in USD |
|
Gastric Sleeve |
$4600 |
|
Gastric Bypass |
$5000 |
|
Mini Gastric Bypass |
$5000 |
|
SADI-S |
$5699 |
Note: The cost of surgerybe different for each person. Things like the type of surgery and your health can change the price. Click the button to get a price for your surgery.

Achieve Weight Loss Success with Obesity Surgery in Tijuana, Mexico

Dr. Maytorena and his team are here to help you get healthier and feel better. He works with experts who know a lot about food, how we think, and how to move our bodies. They want to help you lose weight in a safe way. Dr. Maytorena knows that surgery is just one part of the process. After the surgery, he will help you stay on track so you can keep the weight off and feel good for a long time. His goal is to help you feel your best!
FAQs (Frequently Asked Questions)

Obesity Bariatric Surgery by Dr. Jorge Maytorena, Tijuana, Mexico Profile Details
Accredited Bariatric Center in Tijuana, Mexico
Dr. Maytorena works at a top clinic in Tijuana that is fully accredited, meaning it meets important safety rules. The clinic is dedicated to providing the best care for weight loss surgery and uses advanced technology to make sure the surgery is safe and effective. You can trust that the clinic has the right tools and equipment to help you on your weight loss journey.
Affordable Weight Loss Surgery in Tijuana
Tijuana, Mexico, is a popular place for people who want weight loss surgery because the cost is much lower than in the United States. Dr. Maytorena and his team offer great care for a fraction of the price. You’ll still receive high-quality treatment, and it can be a great option for those looking for affordable surgery options.
Advanced Technology for Successful Obesity Surgery in Mexico
At Dr. Maytorena's clinic, they use the latest technology to make sure weight loss surgery goes smoothly. Tools like robotic surgery and small cameras help the doctors perform surgeries more accurately, which leads to a faster recovery and less pain. The team is always working to make your experience as easy and safe as possible.
Obesity Bariatric Surgery by Dr. Jorge Maytorena Treatments Offered
Our Comprehensive Bariatric Surgery Procedures in Tijuana, Mexico
Dr. Maytorena offers a range of advanced surgical techniques for weight loss, including:
Dr. Maytorena works with each person to find the best surgery for them. Look at the pictures to see how he has helped people.
Before and After Image of Bariatric Surgery in Tijuana, Mexico
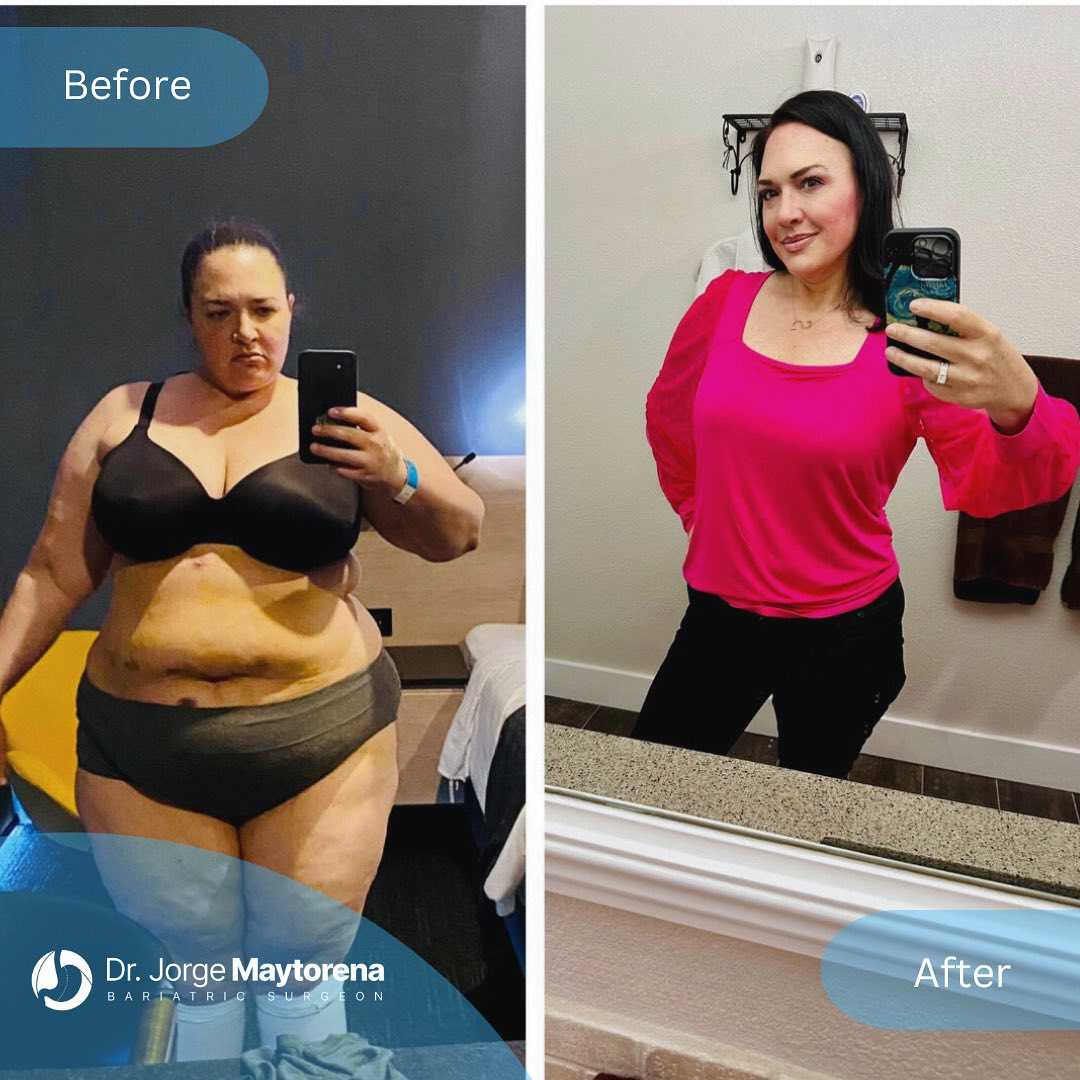
Before and After Image of Obesity Surgery in Tijuana, Mexico

Before and After Image of Weight Loss Surgery in Tijuana, Mexico

Before and After Image of Weight Loss Surgery in Tijuana, Mexico

Before and After Image of Bariatric Surgery in Tijuana, Mexico

Before and After Image of Gastric Sleeve Surgery in Tijuana, Mexico

Before and After Image of Bariatric Treatment in Tijuana, Mexico

The best weight loss doctors in Tijuana use the latest tools and methods to help people get the results they want.
Obesity Bariatric Surgery by Dr. Jorge Maytorena Certificates, Accreditations, Qualifications Treatments Offered
Highly Qualified Bariatric Surgeon in Tijuana, Mexico
Dr. Jorge Maytorena is a weight loss doctor in Tijuana, Mexico. He is very good at his job. He knows a lot about weight loss surgery. He makes a special plan for each person he helps. He uses the best ways to do surgery. He wants his patients to be safe and healthy.

Dr. Jorge Maytorena
Dr. Maytorena really cares about his patients. He wants to help them learn about how to be healthy. He wants them to feel good for a long time. He is known for being a great doctor.
Obesity Bariatric Surgery by Dr. Jorge Maytorena Testimonials
Successful Weight Loss Journeys with Dr. Jorge Maytorena in Tijuana, Mexico
Many people have had weight loss surgery with Dr. Jorge Maytorena. They have lost a lot of weight and feel much better. They talk about how Dr. Maytorena helped them and cared for them. They are very happy with their surgery.
Ed Rocha Testimonial
Andrea Testimonial
People who had surgery with Dr. Maytorena are very happy. They are healthier and feel better. Their stories can help other people who want weight loss surgery. They can see how it is possible to live a healthier life.
Luz Anahi Estrada Ames
Ina Mercy Marfil Massa
Tammie Gibson
Mike Agulera
Obesity Bariatric Surgery by Dr. Jorge Maytorena Awards & Recognitions
Dr. Jorge Maytorena: Certified Bariatric Surgeon in Tijuana, Mexico
Dr. Jorge Maytorena and his team have won many awards. They are known for being really good at helping people. They have a special hospital in Tijuana, Mexico. They are very good at weight loss surgery and helping people look better. They have won awards because they work hard to keep people safe.
Dr. Jorge Maytorena, Certified Bariatric Surgeon
Certified Bariatric Surgeon, Expert in Weight Loss
Dr. Maytorena: Trusted Certified Bariatric Surgeon
Patients choosing Dr. Jorge Maytorena can be assured of receiving top-tier treatment in a supportive and technologically advanced environment, ensuring their journey towards improved health and enhanced well-being is met with unparalleled expertise and care.
Tijuana, Mexico Destination Overview

Medical Tourism for Bariatric Surgery in Tijuana, Mexico
Tijuana is a great place to visit for weight loss surgery. It is close to the United States, has excellent hospitals, and costs less than having surgery in the United States. Many people go to Tijuana each year for surgery. This guide will help you plan your trip. It tells you how to get there, what to expect, and fun things to do in Tijuana.
Getting to Tijuana, Mexico
You can get to Tijuana by plane, bus, car, or ship.
Documents Needed
Top Tourist Attractions in Tijuana
Tijuana has many fun places to visit! You can go to a big museum, see a movie, and look at cool things. There is a street with lots of shops and places to eat. You can learn about the history of the area at a museum. You can also relax at the beach. There is a big park with a zoo and a lake. You can buy food and other things at a market. There is also a shopping mall with stores and restaurants. And don't forget to try the yummy food in Tijuana!.
Practical Tips
Tijuana is a great place to have weight loss surgery. It has excellent hospitals and doctors. You can also have fun in Tijuana! There are many things to see and do. Make sure you have all your important papers. Then, you can enjoy your trip and have a great time in Tijuana.
Location
Reviews

Dr. Maytorena is amazing. He is so professional, kind and nice. He makes you feel in good hands, and believe me you are in amazing hands. My surgery has been the best decision of 2023.
Abril
Google Aug 16 2023
Recommended100% the best decision, the best team
Leandro
Google Aug 17 2023
Excellent Dr, I have been operating for 5 years without any problem and above all a spectacular change in my life, 100% recommended
eduardo
Google Sep 29 2023About Medical Center
- Translations: EN ES
- Speciality: Obesity/Bariatric Surgery, Weight Loss Program, Laparoscopic Surgery
- Location: Dream's Hospital. Gobernador Ibarra 9721, Americas , Tijuana 22044 , Mexico
- Packages: Gastric Sleeve Package in Tijuana, Mexico by Dr. Jorge Maytorena , Dr. Jorge Maytorena Gastric Bypass Package in Tijuana, Mexico , Mini Gastric Bypass in Tijuana, Mexico by Maytorena , Laparoscopic Gall Bladder Removal in Tijuana, Mexico ,
- Medically reviewed by: Dr. Jorge Maytorena
- Last Reviewed: 2026-03-04
- Author Name: Hina Munawar
- Associated Doctors: Dr. Jorge Maytorena
- Medical Center Videos: Obesity Bariatric Surgery by Dr. Jorge Maytorena
- Medical Center Prices: Obesity Bariatric Surgery by Dr. Jorge Maytorena
- Overview: Dr. Jorge Maytorena is among the best weight loss doctors in Tijuana, Mexico. Seek expert obesity care at his accredited Cosmetic & Bariatric Surgery Center.





.png)
.png)
.png)
.png)










Share this listing