Dealing with severe follicular depletion requires a highly strategic approach to hair restoration. Patients experiencing extensive baldness often struggle to find viable clinical solutions. Securing an advanced hair transplant procedure in the United States requires navigating complex surgical techniques and assessing highly limited donor resources.
A very common scenario that surgeons encounter is a [00:00] patient who shows up for consultation with extremely advanced hair loss. These cases demand a deviation from traditional graft harvesting methods. Physicians must rely on specialized extraction protocols to maximize the available genetic material.
This comprehensive guide examines the precise methodologies used to treat the most advanced stages of male pattern baldness. We will break down the clinical parameters of severe follicular depletion and outline the surgical pathways available for individuals with minimal donor capacity.
Video Chapters
- Understanding the Norwood Scale Progression
- Defining the Norwood 7 Hair Loss Pattern
- Evaluating Finite Donor Area Capacity
- Strategic Overharvesting in Hair Restoration
- FUE Hair Transplant for Extensive Balding
- Camouflaging FUE Punch Marks Effectively
- Setting Realistic Hair Restoration Expectations
- Post-Operative Care for Extensive FUE Sessions
Understanding the Norwood Scale Progression
The Norwood scale remains the standard medical classification system for measuring male pattern baldness. Doctors use this diagnostic tool to determine the severity of follicular miniaturization across the scalp. Accurate classification dictates the specific surgical approach required for successful grafting.
Pattern baldness typically begins with minor recession at the temples. Without medical intervention, this recession slowly progresses across the frontal band and mid-scalp. Eventually, the vertex or crown begins to thin, creating a distinct separation between the remaining hair zones.
How DHT Impacts Long-Term Follicle Health
Dihydrotestosterone (DHT) serves as the primary biological catalyst for androgenetic alopecia. This hormone binds to specific receptors within susceptible hair follicles. Over several years, the binding process shrinks the follicle diameter and drastically shortens the natural growth cycle.
Once follicles succumb completely to DHT sensitivity, they stop producing visible hair shafts entirely. Only follicles located in the safe donor zone resist this hormonal degradation. Surgeons rely entirely on these DHT-resistant grafts to perform any successful hair restoration procedure.
- Norwood 1 to 3: Characterized by mild to moderate temple recession and early frontal thinning.
- Norwood 4 to 5: Features significant mid-scalp loss and widening of the vertex balding area.
- Norwood 6 to 7: Represents the most severe stages of genetic hair loss with minimal remaining coverage.
Defining the Norwood 7 Hair Loss Pattern
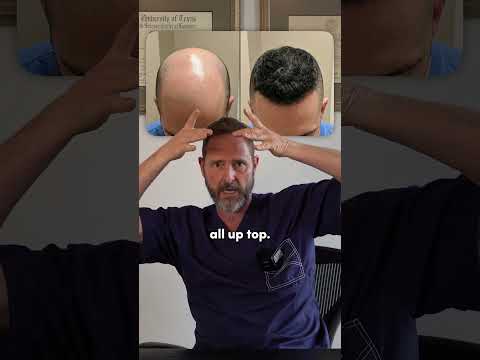
Reaching the final stage of the baldness diagnostic scale presents unique clinical challenges. On the Norwood scale, it would be a [00:07] Norwood 7, which denotes nearly total depletion of the superior scalp. Patients in this category have lost all native hair across the frontal band, mid-scalp, and vertex regions.
The remaining growth creates a highly specific and recognizable visual pattern. That is literally where a horseshoe shape of hair is [00:10] located around the ears and down in the lower neck. This narrow band contains the only permanent, DHT-resistant follicles left on the patient's head.
Structural Characteristics of Severe Depletion
In these extreme cases, there is no hairline remaining to frame the patient's face. There is absolutely nothing on top of the scalp to provide structural coverage or density. Furthermore, the crown actually even dips very low in the back, further reducing the overall surface area of the safe donor zone.
The combination of a vast recipient area and a severely diminished donor region makes standard density targets impossible. Surgeons must completely rethink their distribution strategy to provide any cosmetic benefit. This requires managing patient expectations regarding visual density and scalp coverage.
- Total Frontal Loss: Complete eradication of the anterior hairline and temporal points.
- Extensive Crown Dipping: The balding vertex extends far down the occipital scalp.
- Narrow Donor Band: Only a thin margin of viable follicles remains above the nape.
Evaluating Finite Donor Area Capacity
The fundamental limitation in treating extensive baldness lies within the occipital scalp. Because the bald area is so expansive, there is just a finite amount of donor [00:20] hair available for extraction. Surgeons must calculate the exact number of available follicular units before attempting any extractions.
A healthy donor area typically contains roughly 6,000 to 8,000 lifetime grafts available for safe harvesting. However, a patient at the final stage of pattern baldness may only possess 2,000 to 3,000 viable units. Attempting to cover a massive recipient space with a critically low graft count requires exact mathematical precision.
The Importance of Scalp Laxity and Density
Donor capacity relies heavily on the natural grouping of hair follicles per square centimeter. Patients with higher native density provide more viable two and three-hair grafts for the surgical team. Thicker individual hair shafts also contribute significantly to the illusion of density once implanted.
Surgeons utilize microscopic evaluation tools to measure the density of the horseshoe band. This clinical assessment dictates whether a restorative procedure remains a viable medical option. If the native density falls below acceptable surgical thresholds, the patient may not qualify for conventional grafting techniques.
| Patient Hair Loss Stage | Average Recipient Area Size | Available Donor Grafts |
|---|---|---|
| Norwood 3 (Moderate) | 40 - 60 sq cm | 6,000+ |
| Norwood 5 (Advanced) | 100 - 150 sq cm | 4,000 - 5,000 |
| Norwood 7 (Severe) | 200+ sq cm | 1,500 - 3,000 |
Strategic Overharvesting in Hair Restoration
Traditional extraction protocols mandate leaving adequate density in the back of the scalp to hide the surgical sites. However, extreme baldness requires an entirely different set of surgical rules. There is an option doctors lay out, which is where they technically overharvest [00:25] the remaining donor zone.
In this aggressive approach, the surgical team removes essentially all or as much of this hair as possible. The primary objective shifts from preserving the donor area's appearance to maximizing frontal restoration. The clinical team systematically depletes the horseshoe band to acquire every viable follicle.
Reversing the Baldness Pattern
Once extracted, surgeons take these massive quantities of grafts and put it all up top. The design focuses entirely on creating a new anterior boundary and providing diffuse coverage across the mid-scalp. In other words, the procedure focuses on reversing the established [00:32] pattern of the hair loss.
By moving the genetic material from the sides and back to the superior scalp, the visual dynamic of the face changes entirely. The patient sacrifices the native density of the posterior scalp to frame their face effectively. This specialized technique requires immense surgical skill to prevent massive donor site scarring.
- Maximized Extraction Yield: Pushing graft numbers beyond standard safe harvesting limits.
- Strategic Reallocation: Prioritizing the frontal third of the scalp over the crown.
- Intentional Depletion: Accepting thinness in the donor zone to achieve frontal cosmetic goals.
FUE Hair Transplant for Extensive Balding
Follicular Unit Excision (FUE) stands as the primary surgical modality for executing these massive redistribution cases. FUE utilizes microscopic punches to isolate and extract individual follicular units directly from the scalp tissue. This method avoids the linear scar associated with older strip-harvesting techniques.
During an extensive overharvesting session, a surgeon may extract thousands of units over a multi-day procedure. Using punch tools ranging from 0.7mm to 0.9mm ensures the smallest possible disruption to the surrounding skin. Precise depth control prevents transection and protects the fragile root structures of the precious few remaining hairs.
Managing Tissue Trauma During Extraction
Extracting such a high volume of grafts from a small surface area increases localized scalp trauma. Surgeons must carefully space their extraction patterns to maintain adequate blood supply to the healing tissue. Poor extraction spacing can lead to necrosis or permanent shock loss in the surrounding unharvested hairs.
Advanced clinics utilize specialized tumescent fluids to lift the scalp tissue away from deeper vascular structures. This safety measure protects the dermal blood vessels while allowing for rapid, high-volume extraction. Proper fluid management remains critical when pushing the boundaries of standard FUE capacities.
- Micro-Punch Tools: Utilizing ultra-fine instrumentation to minimize dermal scoring.
- Multi-Day Sessions: Splitting massive extraction numbers across consecutive surgical days.
- Graft Hydration: Storing excised units in chilled holding solutions to ensure survival.
Camouflaging FUE Punch Marks Effectively
Pushing the limits of donor extraction inevitably alters the visual appearance of the occipital region. It is highly possible that FUE punches can be visible [00:35] in this specific overharvested scenario. The tissue heals with tiny, hypopigmented dots that lack native hair coverage.
Patients must adapt their grooming habits to manage this intentional surgical depletion. A completely shaved head using a razor will clearly display thousands of microscopic extraction marks. However, strategic styling easily mitigates this cosmetic byproduct of the procedure.
Utilizing Proper Guard Lengths for Concealment
Concealing the surgical aftermath requires minimal hair growth over the affected areas. For the most part, as long as patients grow the hair around a half or a one [00:40] guard length, the marks vanish. This short buzz cut provides just enough optical coverage to obscure the hypopigmentation.
Under these grooming conditions, the scattered FUE punches are generally very well camouflaged. Observers perceive a short, uniform haircut rather than an aggressively harvested donor zone. Some patients also incorporate Scalp Micropigmentation (SMP) to further darken the depleted areas and reduce contrast against the skin.
- Clipper Guard #1: Leaves approximately 1/8 inch of hair length for optimal blending.
- Clipper Guard #0.5: Leaves 1/16 inch of hair, suitable for lighter skin tones.
- Scalp Micropigmentation: Medical tattooing that masks hypopigmented extraction sites.
Setting Realistic Hair Restoration Expectations
Treating severe baldness requires strict alignment between clinical realities and patient desires. A patient starting with extensive loss cannot achieve the dense, thick hair of their youth regardless of the surgical method. The physical math of limited donor supply versus massive recipient demand prevents total restoration.
The goal of an aggressive redistribution strategy is framing the face and creating an illusion of coverage. Surgeons build a conservative, age-appropriate hairline and apply a light dusting of grafts across the mid-scalp. This diffuse coverage eliminates the severe bald appearance without promising impossible density.
Evaluating the Trade-off for Severe Hair Loss
Patients must weigh the benefits of gaining frontal hair against the reality of a severely thinned donor zone. For most individuals suffering from extreme baldness, framing the face holds far more psychological value than preserving the sides. This psychological relief drives the demand for such aggressive surgical interventions.
Ultimately, this specialized redistribution technique is generally a much better alternative [00:50] than remaining completely bald. The improvement in facial framing drastically alters a patient's profile and enhances overall aesthetic symmetry. It transforms a severe balding pattern into a managed, cosmetically acceptable appearance.
- Age-Appropriate Design: Constructing mature hairlines that require fewer grafts to execute.
- Illusion of Density: Shingling grafts strategically to block light from hitting the bare scalp.
- Psychological Relief: Restoring the facial frame to improve patient confidence and self-image.
Post-Operative Care for Extensive FUE Sessions
Recovering from an aggressive overharvesting procedure demands strict adherence to clinical aftercare protocols. The sheer volume of extraction sites increases the surface area of healing tissue exponentially. Patients must keep the donor region immaculately clean to prevent localized bacterial infections.
Surgeons typically prescribe topical antibiotic ointments alongside specialized saline sprays to facilitate rapid dermal repair. Healing times for the massive donor wound area usually span from ten to fourteen days. During this period, patients must avoid excessive physical exertion that could elevate blood pressure and induce bleeding.
Protecting the Newly Implanted Frontal Grafts
While the posterior scalp heals from mass extraction, the recipient area requires extreme physical protection. The newly placed follicles remain highly vulnerable to dislodgement during the first week following surgery. Patients must sleep in an elevated position to prevent accidental friction against pillows or bedding.
Scab formation across the vast recipient zone is a normal physiological response to the micro-incisions. Clinics provide detailed washing instructions to gently loosen and remove these crusts without pulling out the underlying grafts. Following these strict washing regimens ensures optimal graft survival rates for these highly valuable follicular units.
- Elevated Resting: Utilizing neck pillows to keep the newly grafted areas untouched during sleep.
- Saline Hydration: Spraying the recipient sites continuously to promote healthy scab formation.
- Crust Removal: Executing gentle circular massages during showering to clear debris safely.
Ready to Explore Your Hair Restoration Options?
Don't let advanced hair loss dictate your confidence. Connect with leading specialists to evaluate your donor capacity and design a customized surgical strategy tailored to your specific needs.
Get Free QuoteView Full Video Transcript
[00:00] A very common scenario that I encounter is a patient who shows up for consultation with extremely advanced hair loss.
[00:07] On the Norwood scale, it would be a Norwood 7. That is literally where a horseshoe shape of hair is around the ears and down in the lower neck.
[00:15] And there's no hairline, there's nothing on top. And the crown actually even dips very low in the back.
[00:20] So there's just a finite amount of donor. There is an option I lay out, which is where we technically overharvest.
[00:26] In other words, we remove essentially all or as much of this hair as possible and put it all up top.
[00:32] So in other words, we're just reversing it. It is possible that FUE punches can be visible in that scenario.
[00:39] But for the most part, as long as they grow the hair around a half or a one, the FUE punches are generally very well camouflaged.
[00:48] It's generally a much, much better alternative than the Norwood 7 that we were referencing earlier.









.jpg)








Share this listing